- 4192 Devonwood Way, Ashburn, Virginia, 20148
- Helpline: +1 (703) 665-3747
Reconstruction of a Soft-Tissue Defect Following Resection of a Sweat Gland Carcinoma
- Home
- Back to Journal
- Article Details
Abstract
Excision of a scirrhous carcinoma in this female patient had produced a soft-tissue defect involving the lower lip and chin: because primary repair had twice been unsuccessful, the patient was scheduled to undergo plastic reconstructive surgery. The previous surgical procedures had left the patient with incomplete lip closure and resultant difficulties with deglutition and speech. Aesthetic appearance was characterized by disturbances that were extensive and impossible to camouflage. Defect repair was planned using a folded radial forearm flap. To prevent ptosis of the lower lip, the free microvascular pedicled graft was suspended bilaterally on the zygomatic arch using a fascial sling technique. The vermilion border, which was still intact after the previous surgical procedures, was incorporated into the graft. The gingival mucosa of the oral vestibulum was covered with a free mucosal graft. Both the functional and the cosmetic result are highly satisfactory one year and six years after surgery.
Keywords: Cancer – Reconstruction – Lower Lip -Free Radial Forearm Flap
Case Report
In January 2001 a lower-lip tumor was detected in this 70-year-old woman during the course of dental treatment. Following excision, examination of the biopsy specimen revealed a diagnosis of scirrhous carcinoma of the lower lip. At the time of the initial diagnosis, the patient had already been treated for a right-sided renal cell carcinoma in 1995, and other comorbidity comprised arterial hypertension and multinodular goiter, grade III.
Clinical examination revealed an indurated tumor of 3 x 4cm in the plane of the chin. Axillary as well as cervical lymph nodes were palpable bilaterally, and thyroid examination revealed focal autonomy. The treatment plan agreed by the surgical c1inic with the patient was to involve complete tumor resection with primary reconstruction of the defect, bilateral functional neck dissection and axillary lymph node c1earance. Thyroidectomy was scheduled for a later date.
In March 2001 the tumor was excised to a c1ear margin (RO). Tumor resection was complemented by bilateral neck dissection (20 tumor-free lymph nodes right, 21 tumor-free lymph nodes left). A platysma flap prepared during neck dissection with its pedic1e based at the mandible was used to cover the defect [1, 2]. The flap was positioned without tension, and the course of wound healing was unexceptional at first. Histopathological examination disclosed a desmoplastic, blue-cell tumor with superficial tubular growth, and a microcystic adnexal carcinoma (= sclerosing sweat gland carcinoma) was diagnosed.
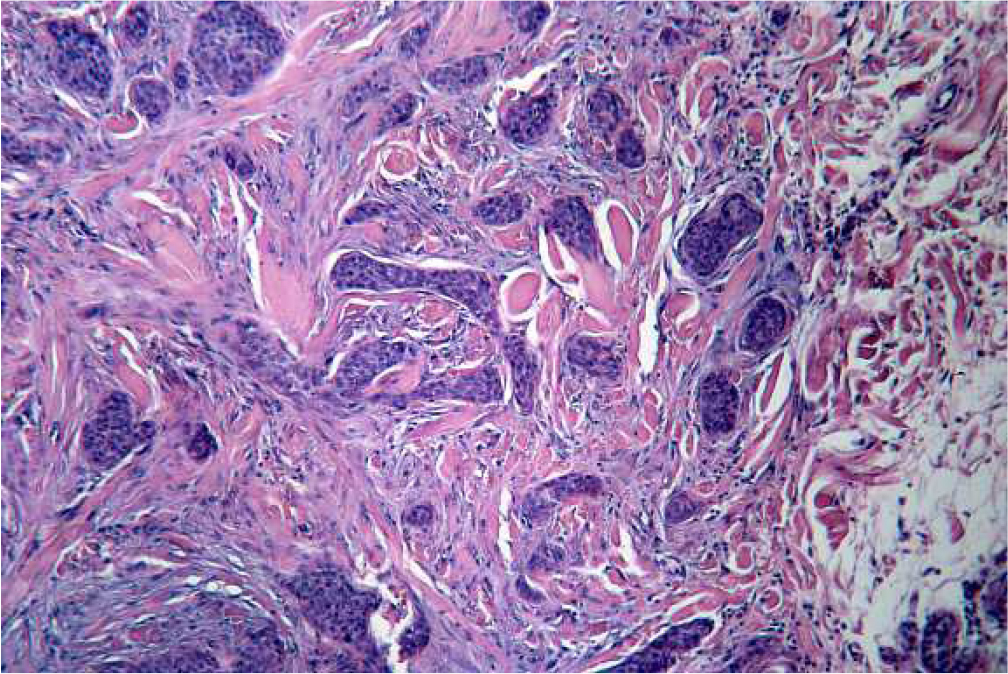
Figure 1: Histology.
In May 2001, 45 days after surgery, a wound-healing disturbance necessitating local measures was noted in the vincinity of the platysma flap. Despite revision, scar contracture developed involving the entire lower lip, which lost its function increasingly over time.

Figure 2: preoperative site (Lower lip distortion and loss of oral vestibule).
Deglutition, speech and facial expression were severely impaired due to non-c1osure of the lips. At the end of August 2001 the original surgeon performed a revision with a mucosal flap from the oral vestibule. The required depth of the oral vestibule could not be achieved by this measure and the functional and aesthetic aspects remained unchanged.
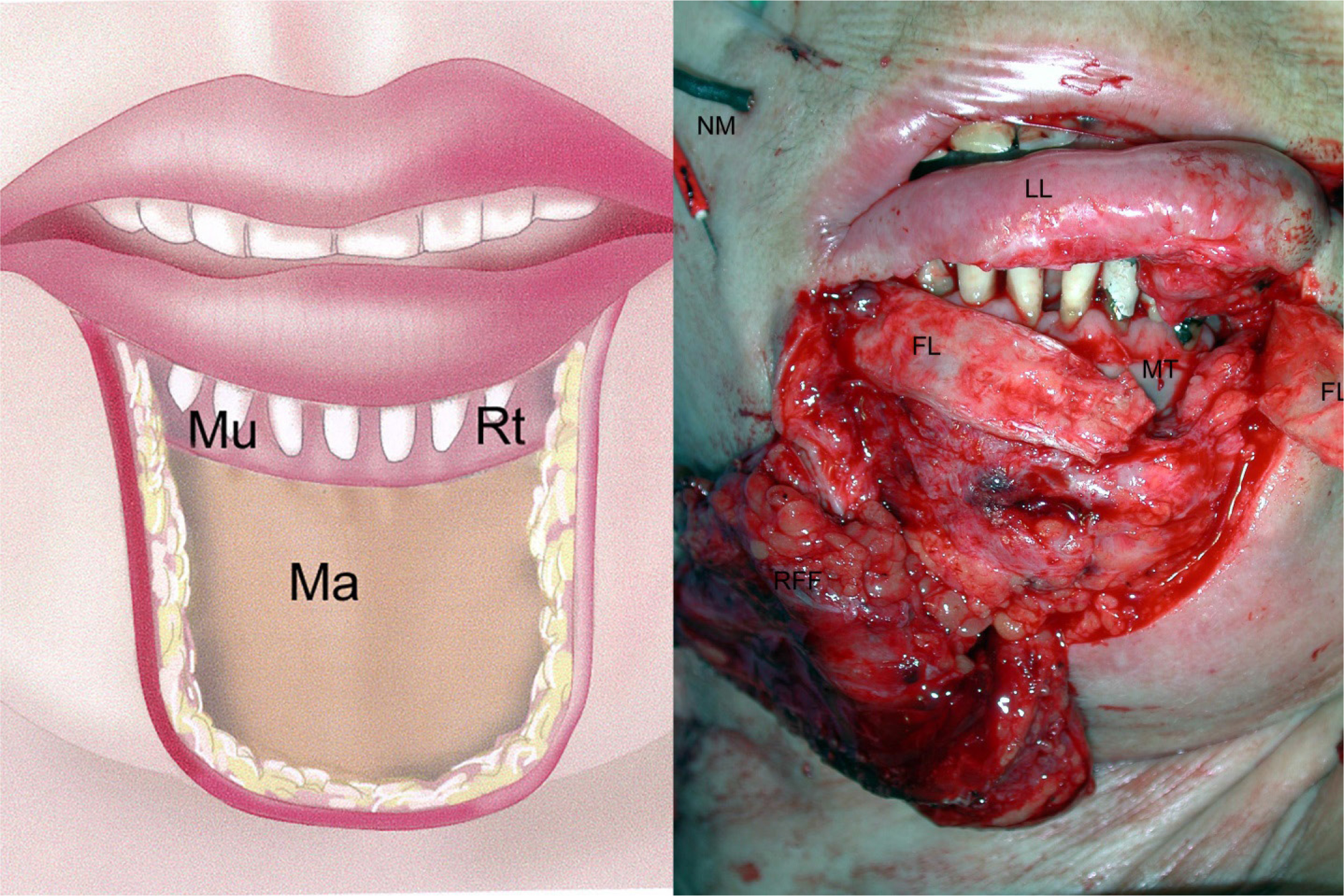
Figure 3: a) Schematic illustration of the resection: Ma = mandible, Mu = mucosa, Rt = root of teeth b) LL = lower-lip vermilion, MT = mucosal graft sutured in place, FL = fascia lata sling, RFF = radial forearm flap, NM = electrodes used for facial nerve monitoring.
The operative strategy involved complete resection of scarring, and replacement of the missing tissue using a 5.5 × 8.5 cm fasciocutaneous radial forearm flap. The lower-lip vermilion was retained as a bridge because it was intact and the continuity of the orbicularis oris muscle could thus be preserved. Particular attention was paid to sparing the facial nerve. Intraoperative neuromonitoring showed that the (facial) nerve was not damaged along its course.
The radial forearm flap was folded cranially and its free ends at the chin were sutured in two layers to the preserved skin of the face. At the cranial convexity a strip of epidermis approximately 1 cm wide was removed, and the vermilion was inserted and attached to the radial forearm flap by two suture lines. The vascular supply of the lip was uninterrupted. Despite the preservation of the oral orbicularis muscle, postoperative alteration of the graft was feared, due in particular to the effects of gravity and of the muscles controlling facial expression. A fascial sling procedure was performed on the lower lip to counteract these effects4. A 5 × 15 cm strip of fascia lata was raised from the thigh, divided lengthwise and positioned in a subcutaneous tunnel from the zygomatic arch to the mandible. It was attached with a resorbable 2x0 suture to the periosteum of the zygomatic arch and sewn along the caudal margin of the radial forearm flap. Deliberate slight over-correction initially caused the patient to smile involuntarily; however, this gave way to a natural facial expression over the course of the first postoperative year.
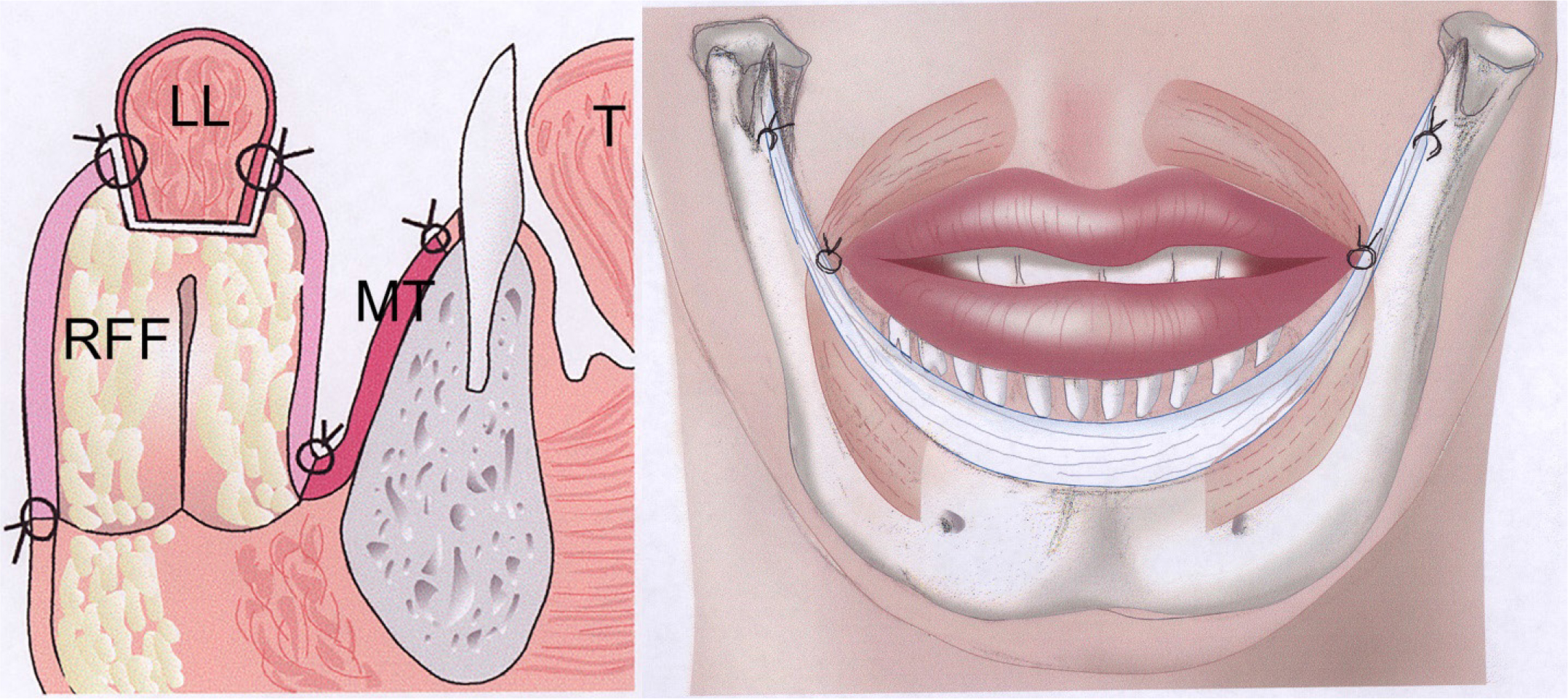
Figure 4: a) Schematic lateral view: T = tongue, RFF = radial forearm flap, MT = mucosal graft, LL = lower lip. 4b) Suspension of the lower lip by fascia.
A free mucosal graft harvested from the intercanthal region of the left cheek was glued to the denuded mandibular regions and was sutured at its margins with the intact buccal mucosa.

Figure 5: a) Immediate postoperative frontal view and b) lateral view at 6 months.
After 2 days’ observation in the intensive care unit, the patient was transferred to a general medical ward. Apart from an adverse reaction to the suture material, the course of wound healing was uneventful. Wound healing by primary intention was accompanied increasingly by a return to normal function, which has continued to the present time.
Discussion
Reconstruction of the facial soft tissues following tumor resection always requires management that is tailored to the individual situation, with the result that generally applicable recommendations cannot be made [5,6]. Local and locoregional flap procedures are usually preferred because they offer promise of maximum textura match, low morbidity at the flap elevation site and good modelling characteristics [1, 6, 7–11]. Myocutaneous platysma flaps [12, 13] and submental island flaps [11, 14, 15] are particularly important for lower-face reconstruction in cases where local rotation and transposition flaps contribute insufficient material to the defect.
We recommend the fasciocutaneous radial forearm flap for use in cases where such procedures are inadequate or where the inherent scarring potential of previous surgery renders local flap procedures disadvantageous [16]. The f1ap is characterized by excellent modelling characteristics, stability, safety and its texture is favourable for the facial region [3]. In contrast with the pectoralis major flap that is also commonly used in the lower face and is a standard graft for reconstructive surgery, the radial forearm flap has definitely superior modelling characteristics and is without disadvantages in terms of safety. The pedic1e of the pectoralis major flap not only commonly produces adverse cosmetic results but is also regularly the cause of graft traction that interferes with function [17].
Despite using a microvascular distant flap technique, the described procedure achieved good graft adaptation to its environment, the sensation of the lower lip in particular was preserved and masticator function was restored.
Acknowledgement
We gratefully thank Frauke Bataille for providing the histopathology images.
References
- Abulafia AJ, Edilberto L, Fernanda V (1996) Reconstruction of the lower lip and chin with local flaps. Plast Reconstr Surg 97: 847–849. [View]
- Bauer T, Schoeller T, Rhomberg M, Piza-Katzer H, Wechselberger G (2001) Myocutaneous platysma flap for full-thickness reconstruction of the upper and lower lip and commissura. Plast Reconstr Surg 108: 1700–1703. [View]
- Shinohara H, Iwasawa M, Kitazawa T, Kushima H (2000) Functional lip reconstruction with a radial forearm free flap combined with a masseter muscle transfer after wide total excision of the chin. Ann Plast Surg 45: 71–73. [View]
- Rose EH (2015) Aesthetic reconstruction of the severely disfigured burned face: a creative strategy for a “natural” appearance using pre-patterned autogenous free flaps. Burns & Trauma 3:16 [View]
- Hayden RE, Nagel TH (2013) The evolving role of free flaps and pedicled flaps in head and neck reconstruction. Curr Opin Otolaryngol Head Neck Surg 21: 305–10 [View]
- Gullane PJ, Martin GF (1983) Minor and major lip reconstruction. J Otolaryngol 12: 75–82. [View]
- Kovacic M (2001) Reconstruction of total lower lip, labial commissure and palatomaxillary defect with composite island cheek flap. Acta Med Croatica 55: 135–139. [View]
- Bayramicli M, Numanoglu A, Tezel E (1997) The mental V-Y island advancement flap in functional lower lip reconstruction. Plast Reconstr Surg 100: 1682–1690. [View]
- Calhoun KR (1992) Reconstruction of subtotal and total defects of the lips. In: Calhoun KR, Stiernberg CM, Bailey BJ, Holt GR (eds.). Surgery of the lip. New York: Thieme Medical Publishers 1992: 42–48. [View]
- Yeo JF, Egyedi P (1988) Reconstruction of soft tissues of the chin and lower lip region following excision ofa basal cell carcinoma. J Craniomaxillofac Surg 16: 337–339. [View]
- Yilmaz M, Menderes A, Barutcu A (1997) Submental artery island flap for reconstruction of the lower and mid face. Ann Plast Surg 39: 30–35. [View]
- Mosche1la F, Cordova A (1998) Platysma muscle cutaneous flap for large defects of the lower lip and mental region. Plast Reconstr Surg 101: 1803–1809. [View]
- Posnick JC, McCraw JM (1988) Reconstruction of the chin-Iower cheek complex with a platysma myocutaneous flap. J Oral Maxillofac Surg 46: 152–155. [View]
- Martin D, Pascal JF, Baudet J, Mondi JM, Farhat JB, et al. (1993) The submental island flap: a new donor site. Anatomy and’ clinical applications as a free or pedicled flap. Plast Reconstr Surg 92: 867–873. [View]
- Prabhune KA, Patni SK, Gomes DA, Bhathena HM, Kavarana NM (1998) The submental .island flap for reconstruction of facial defects. Indian J Cancer 35: 88–93. [View]
- Soutar DS (1989) Radial forearm flaps. In: Baker SR, ed. Microsurgical reconstruction of the head and neck. New York: Churchill Livingstone; 1989: 139–157. [View]
- Schusterman MA, Kroll SS, Weber RS, Byers RM, Guillamondegui O, Goepfert H (1991) Intraoral soft tissue reconstruction after cancer ablation: a comparison of the pectoralis major flap and the free radial forearm flap. Am J Surg 162: 397–399. [View]