- 4192 Devonwood Way, Ashburn, Virginia, 20148
- Helpline: +1 (703) 665-3747
Percutaneous Closure of a Large Coronary Pseudoaneurysm with a Stent Graft – A Case Report
- Home
- Back to Journal
- Article Details
Abstract
Percutaneous intervention is the treatment modality for coronary artery disease. Complications post-intervention can manifest as coronary pseudoaneurysm. Surgery is the usual approach to the management of pseudoaneurysms. We report a large pseudoaneurysm closed percutaneously in a female with unstable angina.
Keywords: coronary artery aneurysm, percutaneous intervention, coronary stent graft, surgery, endoleak
Introduction
Coronary artery aneurysm is a rare complication post percutaneous coronary intervention, with a reported incidence of 0.9% to 6% as per the available literature [1]. Most of the coronary artery aneurysms are pseudoaneurysms [1]. We report a case of large coronary artery pseudoaneurysm managed percutaneously with stent-grafts.
Case
A 67-year-old female with a history of hypertension and diabetes presented with angina of two weeks duration. At admission, her vitals were stable and clinical examination was unremarkable. The 12 lead electrocardiogram did not show any changes suggestive of ischemia. The echocardiography done revealed normal left ventricular function. Her laboratory profile was within normal limits.
Three months before the current admission she had similar complaints for which she was evaluated and was found to have double vessel disease after conventional coronary angiography. Subsequently, percutaneous transluminal angioplasty to both vessels Left Circumflex (LCX) and the Right Coronary Artery (RCA) was done with implantation of stents of size 3.0 X 36 mm Sirolimus-Eluting Stent (SES) (Yukon Choice PC, Translumina, Hechingen, Germany and Translumina Therapeutics, Dehradoon, India) in LCX – OM2 and 3.5*24 mm Sirolimus-eluting stent (SupraFlex, Sahajanand Medical Technologies, Surat, India) in RCA. Post-procedure she was stable and was discharged on dual antiplatelet and statins along with antihypertensive and antidiabetic drugs. She was asymptomatic thereafter and did not follow up there.
Considering her history, she was taken up for repeat coronary angiography through the right radial route which revealed patent stent in RCA, proximal total occlusion of the LCX, and a large coronary artery aneurysm proximal to the occlusion (Figure 1 and 2).
For the better anatomic orientation of the aneurysm, the patient was subjected to Computed Tomographic Coronary angiography, which revealed the aneurysm size to be of 3.5X3.5 cm with thrombus in situ, there was a predominance of calcified stenosis in the second obtuse marginal branch (OM2) (Figure 3). Because of the large pseudoaneurysm, infective etiology was ruled out after two sets of blood culture showed no growth over 48 hours.
The option of surgery – resection of the aneurysm and the graft placement distal to the stent was given to the patient and the attendants because of the large aneurysm and the total occlusion of the left circumflex. They did not opt for surgery and she was taken up for the percutaneous approach. The preferred plan was to place a stent graft across the aneurysm opening and placement of a stent for the in-stent restenosis.

Figure 1: LAO cranial angiographic view of the left coronary system showing large pseudoaneurysm arising just proximal to the stent in the circumflex artery and distal total occlusion.
After bilateral groin preparation and infiltration of local anesthesia, Right femoral arterial and venous access, left side femoral arterial access was taken.7F Cordis (Santa Clara, California, US) sheath was placed in the right femoral artery and 5F sheath in both the right femoral vein and the left femoral artery. The guide catheter used to cannulate the left main coronary ostium was 7F XB 0.018”(Cordis, Santa Clara, California, US) and JR 3.5 Launcher (Medtronic, Minneapolis, Minnesota, US) diagnostic coronary catheter for the right coronary ostium. The total occlusion was crossed with 0.014” ASAHI Sion blue (Vascular Perspectives, Huddersfield, UK) wire over the Finecross microcatheter (Terumo Medical Corporation, Somerset, NJ) into distal LCX artery. Predilation was done with 1.1X10 mm Quantum Maverick (Boston Scientific India Pvt. Ltd) balloon at 12 atmospheres for 15 sec. Distal flow achieved after predilation.
The patient developed angina during the procedure, relieved by intracoronary nitroglycerine (NTG) 150 ug and nicorandil 2 mg. A 2.8 mm * 19 mm Graftmaster stent coronary graft (Abbott Vascular, Santa Clara, California, US) was placed in proximal LCX extending into mid LCX, deployed at 16 atmospheres for 90seconds. Check angiogram showed aneurysm filling from the distal end of the stent-graft. A 2.5 *20 mm Papyrus coronary stent graft (PK Papyrus, Biotronik, UK ) was then placed in mid-LCX overlapping the proximal stent with 5 mm, deployed at 16 atmospheres for 90sec. A check angiogram showed tiny leaks into the aneurysm. Further stent-graft deployment was deferred. The distal LCX stent with in-stent restenosis was covered by Resolute Onyx 2.25 *38 mm (Medtronic, Minneapolis, US) deployed at 12 atm for 30 sec. Post dilation of the stent was done with a 2.5*12 mm balloon at 16 atmospheres for 10 seconds. The stent-grafts were post dilated with 3.5 *8 mm Apollo balloon (BrosMed Medical Co., Ltd., Dongguan, China) at 12 atmospheres for 10 sec. The Type I endoleak persisted. Distal LCX showed TIMI III flow (Figure 4). The vascular access was closed by Abbott Perclose (Abbott Vascular, Santa Clara, California, US).

Figure 2: AP caudal view of the circumflex artery showing large pseudoaneurysm.
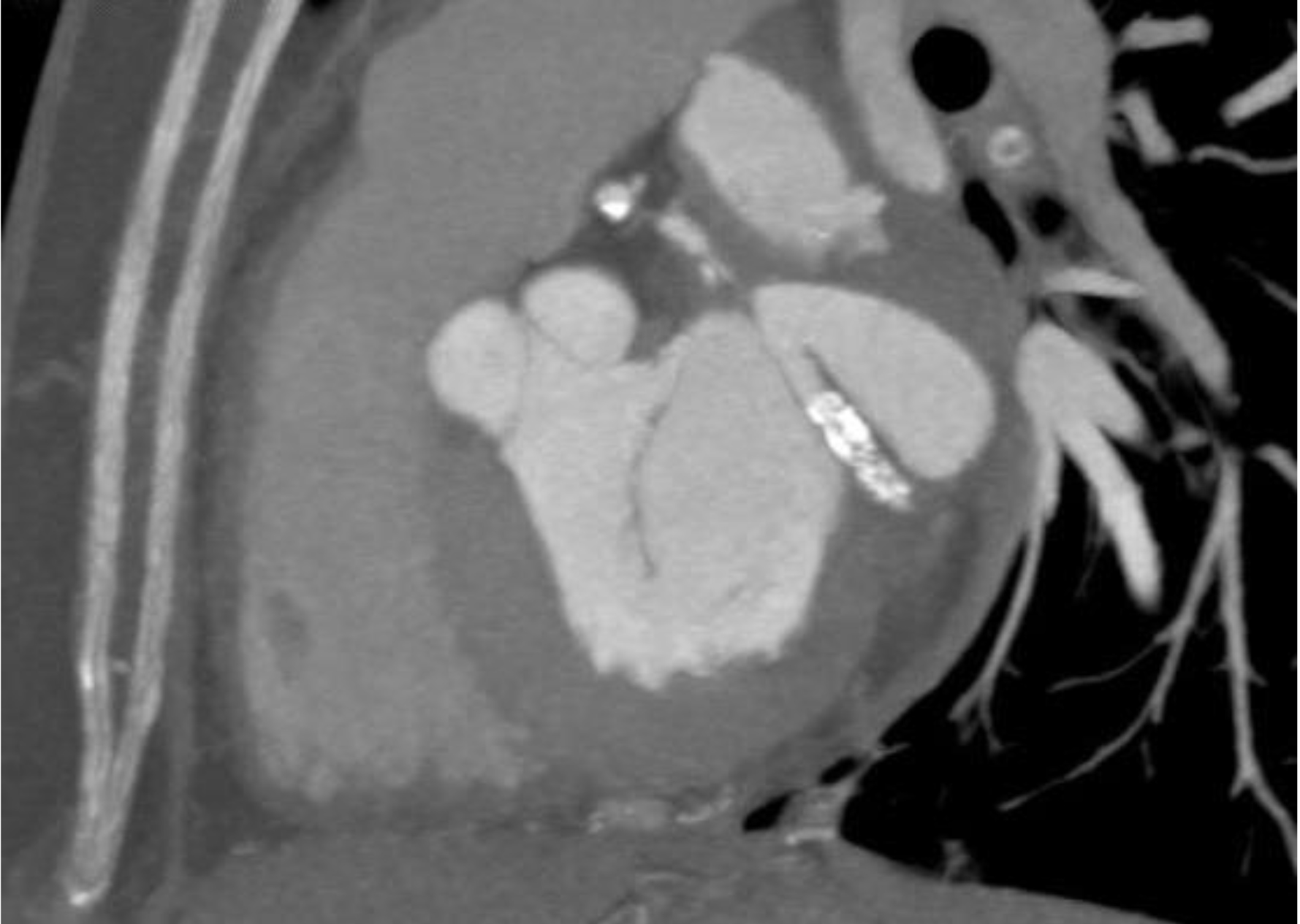
Figure 3: Computed tomography image showing the pseudoaneurysm and calcified lesion within the stent in the circumflex artery.

Figure 4: post-intervention small leak into the aneurysm is seen.
The patient was discharged on dual antiplatelet and high dose statins (Ticagrelor 90mg bd and Aspirin 75 mg OD, Atorvastatin 80 mg OD). CT coronary angiography at follow up showed no leak into the aneurysm, the aneurysm was thrombosed (Figure 5). She was asymptomatic and was advised the same medication to continue.
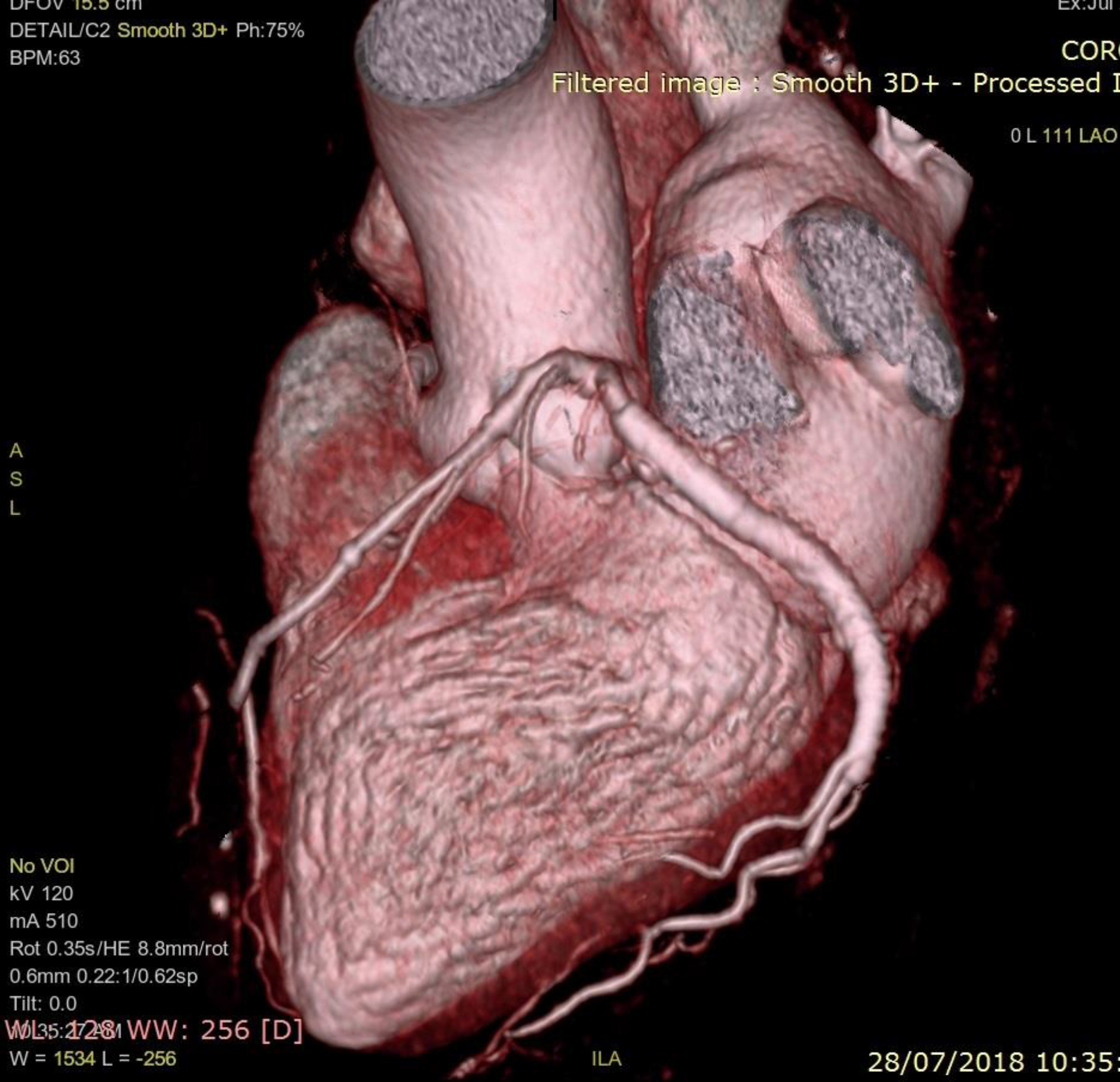
Figure 5: Three dimensional volume rendered computed tomography image of the heart showing the absence of the pseudoaneurysm and patent stent in the left circumflex artery.
Discussion
Pseudoaneurysm formation post percutaneous intervention is rare and is secondary to the injury caused to the artery as a result of the stent deployment or the drug impregnated to the stent [2–4]. Stabile et al have suggested that there can be a patient-specific sensitivity to sirolimus leading to aneurysmal dilation and aneurysm formation [2]. Coronary angiography cannot differentiate between the aneurysm and pseudoaneurysm and requires intravasular imaging [3]. On intravascular ultrasonography, it has been shown they are associated with large atheroma burden indicating them to be secondary to atherosclerosis. The stent malapposition and edge dissection of the stents were considered as contributing factors.[3, 5]. To our best knowledge, this is the first case to be reported in the literature of successful closure of large pseudoaneurysm with stent-graft.
Learning Objectives
Coronary pseudoaneurysms is secondary to the stent edge dissection after intervention. Small aneurysms can be approached percutaneously or managed medically based on the clinical features. Surgery is preferred in large aneurysms though can be intervened percutaneously on an individual basis with good results as seen in this case.
Conclusion
In selected cases with heart team approach coronary pseudoaneurysms can be intervened percutaneosuly.
References
- Wang KY, Ting CT, St John Sutton M, Chen YT (1999) Coronary artery aneurysms: A 25 patients study. Catheter Cardiovasc Interv 48: 31–8. [View]
- Stabile E, Escolar E, Weigold G, Weissman NJ, Satler LF, Pichard AD, et al. (2004) Marked malposition and aneurysm formation after sirolimus-eluting coronary stent implantation. Circulation 110: 47–8. [View]
- Berkalp B, Kervancioglu C, Oral D (1999) Coronary artery aneurysm formation after balloon angioplasty and stent implantation. Int J Cardiol 69: 65–70. [View]
- Slota PA, Fischman DL, Savage MP, Rake R, Goldberg S (1997) Frequency and outcome of the development of coronary artery aneurysm after intracoronary stent placement and angioplasty. STRESS trial investigators. Am J Cardio 79: 1104–6. [View]
- Aoki J, Kirtane A, Leon MB, Dangas G (2008) Coronary artery aneurysm after drug eluting stent implantation. J Am Coll Cardiol Intv 1: 14–21. [View]