- 4192 Devonwood Way, Ashburn, Virginia, 20148
- Helpline: +1 (703) 665-3747
Mechanical Ventilation in the Prone Position for Patients with COVID-19 Infection: A Therapeutic Alternative in Spontaneous Ventilation
- Home
- Back to Journal
- Article Details
Introduction
In December 2019, a new coronavirus was attributed as the causative microorganism for documented atypical pneumonia in a province of Wuhan, China, and after genetic sequencing, it was named SARS-CoV 2 for the structural and genomic similarity to another coronavirus, SARS. -CoV [1]. The high transmissibility of the virus led to its rapid expansion worldwide, causing the COVID-19 disease that was declared a pandemic for March 2020, and today represents a public health challenge due to the high mortality of patients who develop the severe form of the disease, with a high requirement for intensive care unit management and the need for invasive mechanical ventilation [2].
SARS-CoV-2, a single-stranded RNA enveloped virus [3], causes a heterogeneous disease known as COVID-19 that presents a wide variety of clinical manifestations ranging from asymptomatic individuals, mild respiratory symptoms with general symptoms such as fever and general malaise, up to severe manifestations that trigger multi-organ involvement and finally death [4]. Among the severe manifestations, severe Acute Respiratory Distress Syndrome (ARDS) caused by the pulmonary disease of the virus is the most common, occurring in 20–41% of patients [5].
Materials and Methods
A search of the literature in PubMed was carried out using “COVID-19; position prone”. We found 59 publications of which 22 articles with relevant content were selected for this review.
SARS-CoV-2 Induced Lung Injury
ARDS was first described in 1968 in patients with pneumonia, sepsis, or trauma as a severe lung compromise clinically manifested by the presence of hypoxemia, non-cardiogenic pulmonary edema, increased respiratory work, and the vast majority of these patients required positive-pressure ventilation [6]. In 2012, the Berlin criteria that currently govern the definition and classification of ARDS according to four criteria emerged: 1. The clinical criteria defined by a time of evolution of respiratory symptoms of one week of evolution; 2. The radiological criteria given by the presence of bilateral opacities that are not explained by effusions, lung collapse or nodules; 3. The presence of pulmonary edema not fully explained by heart failure or volume overload and, finally, 4. The criterion depending on the oxygenation variables that classifies ARDS in three groups: mild when the PaO2 / FiO2 is between 200–300 mm Hg with a PEEP of > 5 cm H2O, moderate when the PaO2 / FiO2 is between 100–200 mm Hg with a PEEP of > 5 cm H2O, and severe when the PaO2 / FiO2 is below 100 mm Hg with a PEEP of > 5 cm H2O [7].
On the other hand, two different phenotypes have been described for patients with ARDS with a variable response to medical management; phenotype 1 to which those patients with stable hypoxemia belong, without the presence of multiple organ dysfunction; and phenotype 2, which are those individuals who develop an acute inflammatory response, refractory hypoxemia with multiple organ dysfunction syndrome, shock and high mortality. Depending on the type of phenotype that the patient presents, they will respond differently to medical management strategies such as mechanical ventilation and fluid therapy, with better results in terms of mortality in patients with sub-phenotype 1 [8, 9].
COVID-19-induced lung injury, especially in the context of ARDS, is variable in presentation and may manifest as classic ARDS, described by the Berlin criteria mentioned above, or may include an atypical presentation where pulmonary compliance is preserved and refractory hypoxemia is multifactorial in etiology. Classically, the pathophysiological bases of COVID-19 that ultimately lead to acute ventilator failure have been grouped into five categories: the first group presenting with the typical pneumonia described in patients with COVID-19 infection, bibasal pneumonia in a ground-glass pattern; the second group are patients who develop disseminated intravascular coagulation that generates micro vascular phenomena of thrombosis in the pulmonary capillaries contributing to hypoxemia; the third group, those patients who develop thrombi located at the level of the pulmonary arteries in the context of pulmonary thromboembolism; the fourth group are patients who develop cardiac injury in the context of COVID-19 with the secondary appearance of pulmonary edema; and finally, a fifth group of patients who develop central nervous system compromise with ventilator failure of neuromuscular origin [10].
Regarding the two phenotypes that have been classically described in patients with ARDS, they are also well differentiated in patients with COVID-19 and pulmonary involvement; the sub-phenotype classically known as phenotype 1, in the context of COVID-19 disease it has been reported as the “L” phenotype (Light or Low). This belongs to the group of patients with little compromised lung compliance, which implies a better response to therapeutic maneuvers; and the classic sub-phenotype 2 corresponds to the H (High) phenotype in COVID-19 disease, a group of patients with compromised lung compliance who respond poorly to the mechanical forces applied in ventilation maneuvers [11].
The mortality of patients who have ARDS due to COVID-19 is high and, because there are no therapeutic measures with sufficient evidence for the management of viral infection, the treatment of respiratory dysfunction includes invasive mechanical ventilation in protective mode with low lung volumes as a support measure, and within this, the prone position is shown as an effective alternative that improves oxygenation parameters and reduces pulmonary edema with results that impact mortality [12, 13].
Mechanical Ventilation in Prone Position in Covid-19 Infection
Invasive mechanical ventilation in protective mode with low lung volumes, ventilation in the prone position and the use of a neuromuscular relaxant such as cisatracurium are the three measures that, in light of the evidence, are more effective in the management of ARDS [14]. In the context of COVID-19 infection, where therapeutic alternatives that have an impact on mortality have been sought, ventilation in the prone position has shown improvement in oxygenation parameters in patients with ARDS who require mechanical ventilator support [15].
The pathophysiological basis of the use of the prone position during ventilator support is that this position favors the ventilation-perfusion relationship in the dorsal areas of the lung, making it more homogeneous, favoring recruitment and gas exchange due to the release of the compression generated by the weight of the abdominal and mediastinal cavity [16] (See Figure 1). It also generates a decrease in pulmonary over distension with cyclic alveolar recruitment, generating a lower risk of ventilator-induced lung injury since any eventual damage caused by the energy load of mechanical ventilation will be distributed more uniformly to the lung parenchyma, impacting positive in the mortality of these patients [17, 18].
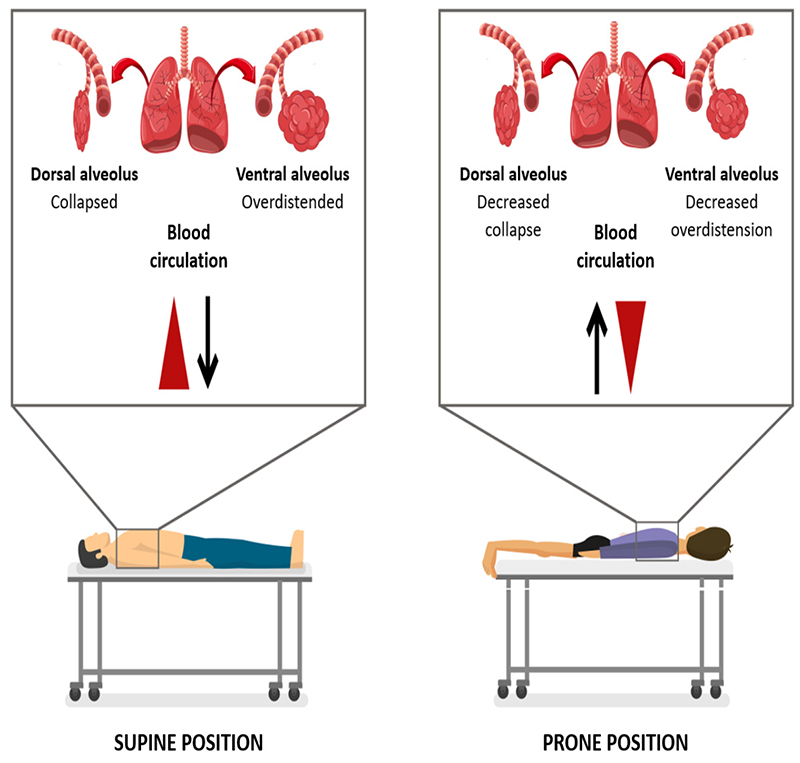
Figure 1. In the course of the current COVID-19 pandemic, where therapeutic measures that impact mortality are required, the ventilation strategy in the prone position early, in the first 24–36 hours, has become a therapeutic alternative in individuals with moderate to severe ARDS that require invasive mechanical ventilation and even in patients during spontaneous ventilation as it improves oxygenation in declining areas of the lung and allows an improvement in clinical results [13, 19, 20]
The importance of the prone position in awake patients and in spontaneous ventilation during COVID-19 disease lies in the decrease in the need for orotracheal intubation, in addition to the reduction in the percentage of admission to the intensive care unit. There have been reports that describe the benefit of using the prone position in patients with spontaneous ventilation, not intubated, in management with standard oxygen supplement, CPAP or NIV, improving oxygenation and decreasing respiratory effort in addition to reducing the risk of self-induced lung injury [20]. The different studies carried out in heterogeneous populations affected by COVID-19, such as the PRON-COVID study, show the improvement in oxygenation parameters in a sustained manner over time, as well as a reduction in the requirement for mechanical ventilation and the days of stay in intensive care unit making it a non-invasive therapeutic alternative for patients with moderate to severe ARDS by COVID-19.
Conclusion
The current pandemic caused by COVID-19 disease has created a new challenge for public health and has forced clinicians to seek therapeutic alternatives that reduce mortality and require an intensive care unit. In this order of ideas, the prone position during spontaneous and assisted ventilation in patients with acute hypoxemic respiratory failure becomes a therapeutic option for patients with moderate to severe ARDS with a positive impact on the improvement of oxygenation and mortality rates due to COVID-19.
References
- Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. [2020] Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 395: 507–513 [View]
- Guan W, Ni Z, Hu Y, Liang W, Ou C, He J, et al. [2020] Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 382: 1708–1720 [View]
- Lu R, Zhao X, Li J, Niu P, Yang B, Wu H, et al. [2020] Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet 395: 565–574. [View]
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. [2020] Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. [View]
- Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. [2020] Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA - J Am Med Assoc. [View]
- Dostálová V, Dostál P. [2019] Acute respiratory distress syndrome. Vnitr Lek. [View]
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, et al. [2012] Acute respiratory distress syndrome: The Berlin definition. JAMA – J Am Med Assoc. [View]
- Calfee CS, Delucchi K, Parsons PE, Thompson BT, Ware LB, Matthay MA. [2014] Subphenotypes in acute respiratory distress syndrome: Latent class analysis of data from two randomised controlled trials. Lancet Respir Med. 2: 611–20. [View]
- Famous KR, Delucchi K, Ware LB, Kangelaris KN, Liu KD, Thompson BT, et al. [2017] Acute respiratory distress syndrome subphenotypes respond differently to randomized fluid management strategy. Am J Respir Crit Care Med. 195: 331–338 [View]
- Phua J, Weng L, Ling L, Egi M, Lim CM, Divatia JV, et al. [2020] Intensive care management of coronavirus disease 2019 (COVID-19): challenges and recommendations. The Lancet Respiratory Medicine. [View]
- Gattinoni L, Chiumello D, Caironi P, Busana M, Romitti F, Brazzi L, et al. [2020] COVID-19 pneumonia: different respiratory treatments for different phenotypes? Intensive Care Medicine. 46: 1099–1102 [View]
- Cochrane Library.[2020] Coronavirus (COVID-19): evidence relevant to critical care. Cochrane Database Syst Rev. [View]
- Coppo A, Bellani G, Winterton D, Di Pierro M, Soria A, Faverio P, et al. [2020] Feasibility and physiological effects of prone positioning in non-intubated patients with acute respiratory failure due to COVID-19 (PRON-COVID): a prospective cohort study. Lancet Respir Med. [View]
- Tonelli AR, Zein J, Adams J, Ioannidis JPA. [2014] Effects of interventions on survival in acute respiratory distress syndrome: An umbrella review of 159 published randomized trials and 29 meta-analyses. Intensive Care Medicine. 40: 769–87 [View]
- Guérin C, Reignier J, Richard JC, Beuret P, Gacouin A, Boulain T, et al. [2013] Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 368: 2159–68. [View]
- Albert RK, Hubmayr RD. [2000] The prone position eliminates compression of the lungs by the heart. Am J Respir Crit Care Med. 1: 1660–5. [View]
- Koulouras V, Papathanakos G, Papathanasiou A, Nakos G. [2016] Efficacy of prone position in acute respiratory distress syndrome patients: A pathophysiology-based review. World J Crit Care Med 5: 121–36. [View]
- Gattinoni L, Busana M, Giosa L, Macrì MM, Quintel M. [2019] Prone Positioning in Acute Respiratory Distress Syndrome. Seminars in Respiratory and Critical Care Medicine. 5(14): 289. [View]
- Liu Y, Sun W, Li J, Chen L, Wang Y, Zhang L, et al. [2020] Clinical features and progression of acute respiratory distress syndrome in coronavirus disease 2019. medRxiv. [View]
- Ding L, Wang L, Ma W, He H. [2020] Efficacy and safety of early prone positioning combined with HFNC or NIV in moderate to severe ARDS: A multi-center prospective cohort2 study. Crit Care. [View]