- 4192 Devonwood Way, Ashburn, Virginia, 20148
- Helpline: +1 (703) 665-3747
COVID-19 War Games in the Caribbean – Round One
- Home
- Back to Journal
- Article Details
Abstract
Purpose: We describe the Novel Coronavirus Disease (COVID-19) pandemic, the public health interventions, clinical management and outcomes in the Caribbean during “Round One” using public data. This is a diverse 44.2 million population from 44 countries/territories in 700 islands with high rates of co-morbidities. The Caribbean hosts 14 of the 15 most tourism-dependent nations in the Americas and five of the top ten tourism-dependent countries world-wide. COVID-19 arrived there on March 01, 2020.
Epidemic control: Caribbean leaders quickly, decisively and collaboratively closed international borders to travelers and implemented strict in-country and within-community public health measures. Suspect cases were evaluated for severe acute respiratory syndrome coronavirus (SARS-Co-V 2) by wide-spread naso-pharyngeal sampling and Polymerase Chain Reaction (PCR) testing with rapid turn-around of results. This allowed aggressive contact tracing of suspect, or confirmed cases which were contained in home, or state-based isolation, or quarantine for 14 days. Patients with severe or critical disease were managed in hospitals, usually repurposed with the requisite administrative and engineering controls.
Outcomes: As of July 8, 2020, thirty-three Caribbean countries/territories reported 67,765 PCR-confirmed COVID-19 cases and 1,383 deaths. The majority (> 57%) were in one country/territory. Trends of COVID-19 cases and deaths show “flattening of the curve” in Cuba, Barbados, Trinidad, Jamaica, Belize and St Lucia and “no new cases for over 14 days” in Anguilla, Bahamas, Bermuda, Bonaire, British Virgin Islands, Dominica, Montserrat, Saba, St Barthelemy, St Pierre and Miquelon, St Eustasius, Grenada, St Vincent and the Grenadines.
Conclusion: The Caribbean halted SARS-CoV-2 importation and onward community spread in “Round one”. It is now embarking upon phased, re-openings of international borders and communities, while implementing in-country public health protocols, amidst COVID-19 surges in North, Central and South America, as it aims to “balance Caribbean lives with their livelihoods”.
Keywords: COVID-19, SARS-CoV-2, Pandemic, Caribbean, Tourism, Jamaica, Contact Tracing.
The Caribbean
The Caribbean’s population of 44.2 million resides in 700 islands, of 44 countries/territories, bordered by land masses of North, Central and South America and the waters of the Caribbean Sea, Gulf of Mexico and Atlantic Ocean. The Caribbean is diverse in its ethnicity, culture, socioeconomic status and language — Spanish (64%), French (25%), English (14%) and Dutch. It is challenged by climate change, hurricanes, earthquakes, arboviral epidemics and the concerns of small island states [1]. The Caribbean’s Tourism Dependency Index (TDI) ranges from 84.7% in Aruba to 8.1% in Trinidad [2]. The Caribbean hosts 14 of the 15 most tourism-dependent nations in all the Americas and five of the top ten most tourism-dependent nations/countries in the world [2]. It attracts 25 Million visitors each year and 50 Billion USD’s in revenue [3]. Caribbean populations are at-risk for unfavorable COVID-19 outcomes, with 18%-35% having co-morbidities [4]. Vulnerabilities include age >60 years (24%) with diabetes (9%-19%), hypertension (20%-39%), male smoking (10%-33%), obesity (19%-32%), sickle cell disease (0.39–0.63%), cancer and HIV infections [5–7]. This brief report summarizes the Novel Coronavirus Disease (COVID-19) pandemic in the Caribbean and the public health, clinical approaches and outcomes to curtail the “first wave”.
The Epidemic
The first Caribbean case of COVID-19 was identified on March 01, 2020, in a traveler from Italy to the Dominican Republic, where there has been political turmoil; this territory now has the Caribbean’s highest number of reported cases and deaths as of July 8, 2020 [8]. Jamaica, Cuba, Guyana, St Vincent and the Grenadines began reporting index cases March 10 and 11, which coincided with WHO’s announcement of the global COVID-19 pandemic on March 11, 2020, while 118,319 total cases and 4,292 deaths were reported, worldwide [8, 9]. Several other Caribbean countries and territories reported their index cases by March 24, 2020 (Table). By June 30, the WHO had reported 10,185,374 cases with 503,862 deaths from 188 countries/regions [8]. Simultaneously, the Caribbean reported of 55,524 confirmed COVID-19 cases, in 33 countries/ territories and 1,242 deaths; 57% of these cases and 60% of deaths were from one territory [9].
Table: Caribbean PCR+ COVID-19 Pandemic and Country Links to Tourism (% Tourism Dependency Index) Compared for High and Low Incidence Countries: COVID-19 Cases & Deaths, July 8, 2020 [10–12].
|
Country/ Territory |
Population 2020 |
% TDI Tourism 2018 |
Index case in 2020 |
Total |
Covids/Million Pop |
Recoveries |
Deaths |
Deaths/ million |
|
Aruba |
106,766 |
84.7 |
18/3 |
105 |
983 |
92 |
9 |
84 |
|
Antigua & Barbuda |
97,929 |
61.4 |
13/3 |
70 |
715 |
23 |
3 |
31 |
|
Bahamas |
393,244 |
59.4 |
15/3 |
104 |
264 |
89 |
11 |
28 |
|
Barbados |
287,375 |
39.4 |
17/3 |
98 |
341 |
90 |
7 |
24 |
|
Belize |
397,628 |
38.4 |
22/3 |
30 |
75 |
19 |
2 |
5 |
|
Cayman Islands |
65,722 |
25.8 |
12/3 |
201 |
3,058 |
194 |
1 |
15 |
|
Cuba |
11,326,616 |
Unknown |
11/3 |
2,395 |
211 |
2,240 |
86 |
7.6 |
|
Dominica |
71,986 |
48.3 |
22/3 |
18 |
250 |
18 |
0 |
0 |
|
Dominican Republic |
10,847,910 |
22.9 |
01/3 |
38,430 |
3,542 |
19,564 |
821 |
76 |
|
Grenada |
112,523 |
42.4 |
22/3 |
23 |
204 |
23 |
0 |
0 |
|
Guyana |
786,552 |
6.5 |
11/3 |
278 |
353 |
125 |
16 |
20 |
|
Haiti |
11,402,528 |
17.0 |
18/3 |
6,371 |
559 |
2,080 |
113 |
10 |
|
Jamaica |
2,961,167 |
38.4 |
10/3 |
737 |
249 |
599 |
10 |
3.4 |
|
St Kitts & Nevis |
53,199 |
38.6 |
24/3 |
16 |
301 |
15 |
0 |
0 |
|
St Lucia |
183,627 |
56.4 |
13/3 |
22 |
120 |
19 |
0 |
0 |
|
St Vincent/ Grenadines |
110,940 |
39.3 |
11/3 |
29 |
261 |
29 |
0 |
0 |
|
Suriname |
586,632 |
3.2 |
13/3 |
614 |
1,047 |
405 |
15 |
26 |
|
Trinidad/Tobago |
1,399,488 |
8.1 |
12/3 |
133 |
95 |
117 |
8 |
5.7 |
|
Turks and Caicos |
38,666 |
Unknown |
23/3 |
49 |
1,267 |
11 |
2 |
52 |
|
|
|
|
|
|
|
|
|
|
|
World: 188 countries |
7.8 billion |
Not applicable |
Unk |
11,669,259 |
1,496 |
6,586,556 |
539,906 |
69 |
|
Mexico |
128,932,753 |
12.3 |
27/2 |
261,750 |
2,030 |
167,800 |
31,119 |
241 |
|
Brazil |
212,559,417 |
6.1 |
25/2 |
1,623,284 |
7,637 |
1,139,844 |
65,487 |
308 |
|
Canada |
37,742,154 |
Unknown |
23/1 |
105,935 |
2,806 |
71,418 |
9,693 |
349 |
|
USA |
331,002,651 |
Unknown |
21/1 |
2,923,432 |
8,832 |
1,415,302 |
129,963 |
393 |
|
New Zealand |
4,822,233 |
Unknown |
28/2 |
1,187 |
246 |
1,492 |
22 |
4.6 |
Epidemic Control
Caribbean leaders were decisive in preparing for, containing and controlling COVID-19. Preparations began in January, as they worked collaboratively to implement modified guidelines from the World Health Organization (WHO), Pan American Health Organization (PAHO), Caribbean Community (CARICOM), Caribbean Public Health Agency (CARPHA) for case management and control [8, 9, 13, 14, 15]. A multi-pronged approach was used to curtail the spread of COVID-19 and protect the public’s health. Initiatives began before the first cases and deaths were announced in some countries. Surveillance and naso-pharyngeal sampling were done for respiratory illnesses and also in communities, healthcare workers, infirmaries, airports, seaports and correctional facilities. Polymerase Chain Reaction (PCR) testing for severe acute respiratory syndrome coronavirus (SARS-CoV-2) was done [16]. All countries have access to SARS-CoV-2 PCR diagnostic laboratories, whether in-country, or through CARPHA’s regional PCR diagnostic laboratory [9]. PAHO trained laboratory personnel and provided diagnostic reagents and supplies. There is amplification of the envelope, E gene for the pan coronaviruses and the RNA-dependent RNA polymerase, RdRp gene, which is specific for only SARS-CoV-2 [16]. Prompt diagnosis and reporting of test results within 24 hours rapidly facilitated identification, quarantine, isolation and contact tracing of confirmed cases and clusters. There was closure of international borders, seaports and airports to travelers; suspension of schools and social gatherings; “stay-at-home” orders; 12 to 24 hour curfews; establishment of national emergency COVID-19 hotlines; wearing of masks in public spaces, “physical distancing” and hygienic measures. Businesses continued by tele-working. Hospitals strengthened their COVID-19 specific management strategies. The University of the West Indies’ and its hospital (UWI) implemented multidisciplinary educational teleconferences, before the pandemic was announced and continued throughout, with local, regional and international reach, approaching over 27,000 participants [17].
Clinical Management
COVID-19, a pro-coagulant illness, maybe characterized by thrombo-embolism and “pneumonia” [18]. Severe cases, in 20%, may include the “cytokine storm” with acute respiratory distress syndrome, disseminated intravascular coagulation, multi-organ failure, sepsis, shock, myocarditis, pulmonary embolism and death [13,14,19]. The “Coagulopathy”, is heralded by thrombocytopenia and elevated D-dimers, fibrinogen, pro-thrombin, thrombin and fibrin degradation products [20]. While the “cytokine storm” is manifested by immune and other markers, which include high serum ferritin, C-reactive proteins, troponins, pro-calcitonin, interleukins 2,6,7,8,10, tumor necrosis factor alpha, interferon and granulocyte macrophage stimulating factor, where available [21]. Other markers include lymphopenia, neutropenia and eosinophilia. Electrolytes, renal and hepatic health are monitored [13,14]. Hyper-glycaemia, elevation of creatinine phosphokinase and lactate dehydrogenase may occur. Arterial blood gases are monitored [13,14]. Blood cultures may identify septicemia. Serology and viral samples are evaluated, where possible, for viral co-infections. Computerized chest tomography shows characteristic COVID-19 features, ultrasounds manifest thrombo-embolism, while echocardiograms and continuous cardiac monitoring evaluate cardiac health.
Gilead has a licensed agreement to supply remdesivir, recently approved, to 20 low-middle income Caribbean countries [22]. Dexamethasone, also recently approved, is being incorporated into drug regimens for severe disease. High-dose intravenous gammagloblin and aspirin are available for pediatric multi-systemic inflammatory syndrome. Anticoagulation is used as low-dose enoxaparin for prophylaxis and high-dose for the critically-ill with emboli, deep vein thrombosis and high D-dimers. Blood is transfused, as needed. Co-morbidities are managed – statins are used for hypercholesterolemia and ischaemic heart disease; Angiotensin-Converting-Enzyme inhibitors and calcium channel blockers are prescribed for hypertension and cardiac disease and bacterial co-infections are treated with antibiotics based on local anti-biograms. With UWI and country leadership, the WHO’s Solidarity Trial is registered in Jamaica, Guyana, Barbados and the Bahamas [23]. Cuba is researching medications to treat, or prevent COVID-19, including itolizumab, a monoclonal antibody and a biopeptide, both are used for the cytokine storm. The UWI is implementing three additional clinical trials in Jamaica, including convalescent plasma, Caflanone (a flavonoid) and Dolutegravir, Tenofovir, Lamivudine in combination for severe COVID-19. Alternative “patient-directed” anti-inflammatory and immune boosters have included turmeric, ginger, zinc and vitamin C.
Oxygen support is used to maintain target O2 saturation of >92–96% [13,14]. Low flow oxygen, up to 8L/min, is delivered through nasal cannulae, or a non-rebreather face mask. Non-responders are transferred to the Intensive Care Unit (ICU), for high flow nasal oxygen, at 20–60L/min. This delays intubation and prevents escalation to invasive ventilation. If this fails, non-invasive (BiPAP) positive pressure ventilation, or invasive mechanical ventilation is commenced. Patients are nursed in the “awake self-proning position” 12 hours/day and physiotherapy is utilized. Resuscitation and volume assessment are performed, while balancing adequate ventilation with overload, preventing and treating sepsis “distributive shock”. Vasopressors include noradrenalin, or vasopressin. To prevent complications, closed suction is done “in-line”, limiting aerosolisation; mechanical-ventilation-days are shortened to reduce pneumonias. Pressure sores, fever, catheter-associated infections, stress ulcers with gastrointestinal bleeding and coagulation are prevented. Nutritional support, psychosocial counseling, family communication using electronic devices and infection control are implemented.
Infection prevention and control are maintained from triage through discharge [13,14]. Some hospitals have been re-purposed with requisite administrative and engineering controls. Health care workers are risk-stratified and assigned, with training, awareness, task-appropriate personal protective equipment, hygiene, and psychosocial support and testing.
Post hospital discharge, quarantine, or isolation, long-term complications of COVID-19 include depression, fatigue, pulmonary, neurological, among others [19]. Asymptomatic patients are discharged from isolation 14 days after PCR+ test. Symptomatic clients end isolation three days clear, asymptomatic. Critically-ill end isolation, when decided by the team, after three days asymptomatic, with two negative PCR’s. Follow-up is based on clinical course and co-morbidities. Patients are released from the COVID-19 pathway of care after a minimum of 14 days since symptom onset. A seven-day wellness care check is done to ensure mask-wearing, social distancing and hygiene.
Outcomes
As of July 8, 2020, the WHO reported 11,669,259 cases with 539,906 deaths from 188 countries/territories [8]. Simultaneously, 33 countries/territories of the Caribbean reported 67,765 confirmed cases, 30,607 recoveries and 1,383 deaths [9]. One territory, the Dominican Republic, continued reported trends of 57% of cases and 59% of deaths. Trends of COVID-19 confirmed cases and deaths for high incidence/prevalence compared with low incidence/prevalence countries are shown for cumulative reports to July 8 [2, 8, 24] (Table).
Jamaica
In Jamaica, simultaneously, 27,142 tests yielded 745 SARS-CoV-2 PCR positive cases; 30% (227) were imported, 32% (236) were from work-place clusters of young people, 32%(236) were contacts of confirmed cases, 5%(39) had no epidemiological link, likely representing in-country community transmission [25]. Most were female-57% with median age-29 years; 80%/599 recovered and 1.3%/10 died. Children aged < 19 years represented 19% and were mainly identified through contact tracing of adult family members, most were therefore asymptomatic, or mildly symptomatic. Cough, fever, headache, shortness of breath and sore throat were the main symptoms in Jamaica. Anosmia and ageusia were prevalent, gastrointestinal symptoms were not infrequently observed. Among 29 COVID-19 admissions to the University Hospital of the West Indies, all had comorbidities. Median age was 58 years, twelve required intensive care. Six of the seven deaths, occurred in ICU cases. Case investigation and contact tracing is the key to controlling the epidemic. Several hundred contact-tracers work day and night to accomplish these goals. In Jamaica, the parish health departments have investigated all confirmed cases. Contact-tracing identified 591 COVID-19 cases in Jamaica from 4,043 secondary, tertiary and quaternary contacts and over 133 chains of transmission, as shown in figure.
Chains of Transmissions for COVID-19 Cases Identified through Contact Tracing in Jamaica (Figure).
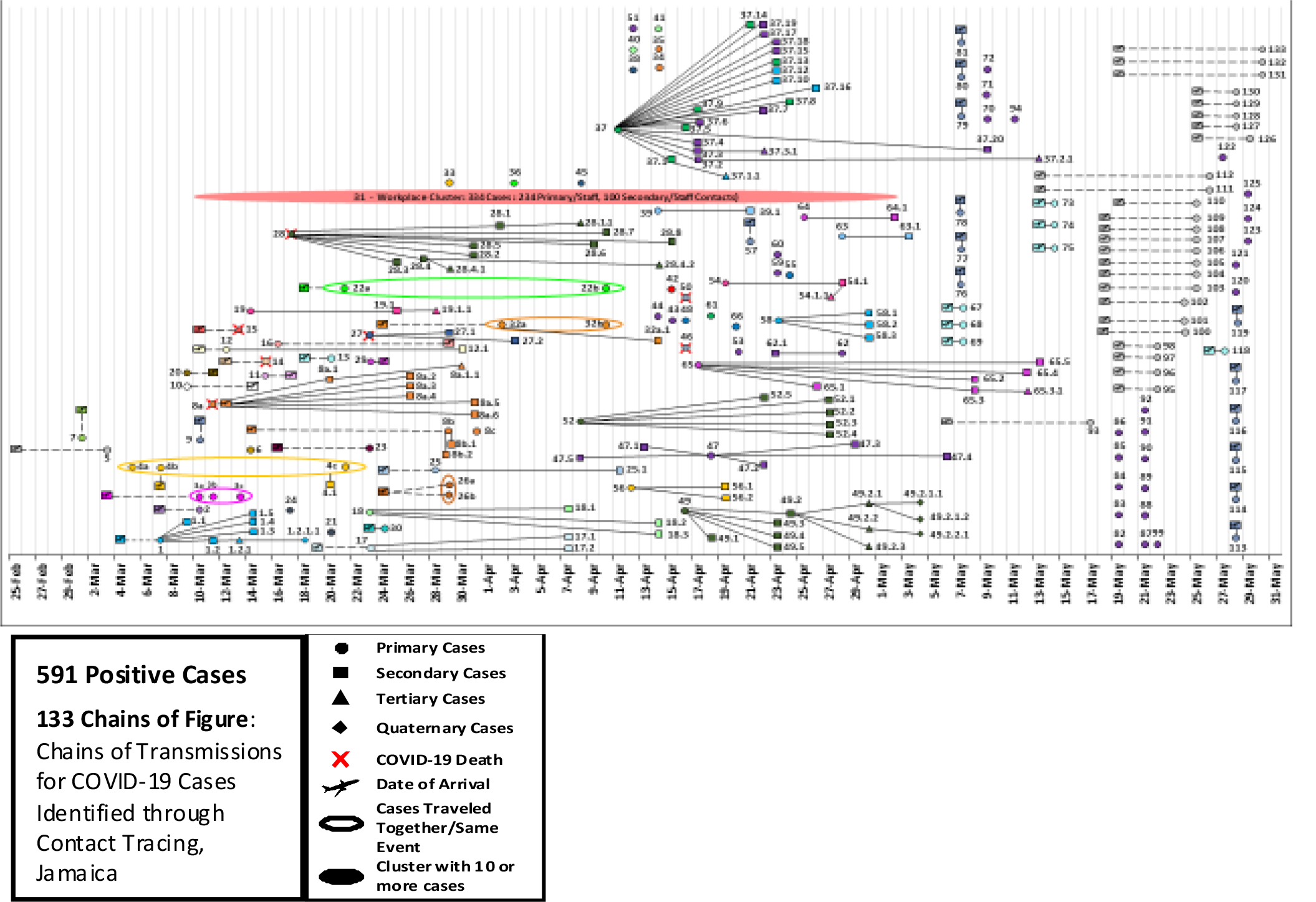
Figure: 591 SARS-CoV-2 PCR-Positive Cases, 133 Chains of Transmission, 4,043 Contacts, 10 Deaths.
Cuba
Cuba demonstrated benevolence, independence and innovation in its response to the Coronavirus pandemic [26,27]. Cuba has the highest ratio of doctors per capita (1:10). There is free universal health care and a well-educated population. Cuba sent a “Medical Brigade” over 1,000 health workers to 18 countries, including to eight Caribbean neighbors. Cuba has a system where hundreds of 1000’s of family doctors, nurses, medical students actively screen all homes for COVID-19, everyday, rapidly identifying persons with COVID-19, contact tracing and quarantine. Everyone who is diagnosed as SARS-CoV-2 positive is hospitalized. Suspect cases are managed in state-run “isolation centers”, for 14 days. There are strict guidelines for isolation and mandatory use of face masks; non-compliant persons are fined, or jailed. Cuba has three SARS-CoV-2 PCR diagnostic labs. Cuba has also been researching medicines for prevention and treatment of Sars-CoV-2. Their monoclonal antibody has significantly cut attributable mortality there.
Haiti
Haiti continues to demonstrate its resilience [28]. While they have received assistance from WHO/ PAHO/ CDC, international aid has been “less than optimal”, in the context of a global COVID-19 pandemic. Haiti closed their international borders, despite the porous borders with Dominican Republic and implemented public health measures to control the epidemic. They have two PCR diagnostic labs. The country remains significantly resource-constrained. While there may be under-reporting, there is a trend towards reduced numbers of cases and deaths. Haiti has given much-needed advice to other similarly severely resource-constrained developing countries [28].
Caribbean
By July 8, trends of COVID-19 cases and deaths in the Caribbean, showed several islands were trending towards ‘flattening the curve’ (eg., Cuba, Barbados, Trinidad, Jamaica, St Lucia, Belize) as compared to “flat-line” in New Zealand Table [8]. While there has been increased cases reported in Suriname, Haiti and the Dominican Republic compared with the surge in Brazil Table [8]. Several other islands/territories have no new cases reported within the previous 14 days, viz., St Barthelemy (99 days), St Pierre and Miquelon (91 days), Anguilla (95 days), Montserrat (85 days), British Virgin Islands (53 days), Saba (43 days), Bonaire (43 days), St Eustasius (43 days), Grenada (42 days), Dominica (25 days), Bahamas (22 days), St Vincent and the Grenadines (20 days), Bermuda (17 days) [8]. Overall, mortality trends show no new cases for several islands, or flattened “mounds” in Belize, Trinidad, Jamaica, Cuba with New Zealand (as a control), with increased deaths in Suriname and Dominican Republic, in comparison to the significant surges in Brazil [8].
Successes
The Caribbean’s early closure of international borders, no doubt, halted importation and onward community spread in the “first round” within the small-island, tourism-dependent states. Collaborative, aggressive and early closure of international borders and early “lock-down” of our communities was done to control COVID-19. Widespread SARS-CoV-2 PCR testing, with rapid turn-around of test results allowed contact tracing, with isolation and quarantine of suspect and confirmed cases, with effective containment of COVID-19. Contact tracing has been outstanding by field staff, with proven prevention of community spread in Cuba and in Jamaica.
Challenges
The main challenge for continued control COVID-19 in the Caribbean is the pre-existing fiscal crises in these primarily small-island states with the unexpected shock to tourism, considering their dependence to sustain these fragile economies [2]. Others include appreciable “at-risk” vulnerable groups with co-morbidities, vulnerable health care systems which may not be able to manage COVID-19 surges. This is compounded by limited access to personal protective equipment, improved rapid diagnostic tests and uniform access to expensive drugs, such as remdesivir [22]. Health care worker fear and anxiety were being addressed. Not all hospitals were administratively prepared to accept patients with COVID-19. Efforts to repatriate Caribbean citizens working on cruise ships were often stymied. The fiscal crisis at PAHO will likely become an issue, shortly, if it is not expeditiously addressed [29]. Other concerns include continuous regional surges of other endemic infectious diseases including dengue, leptospirosis and malaria and the coronavirus outbreak in Haiti and the Dominican Republic, especially on the border [8, 9, 28]. While the WHO’s Solidarity Trial allows controlled use of antiviral drugs, accelerating evidence-based knowledge attainment in developing countries, there were few severe, or critically ill COVID-19 admissions to the region’s hospitals and/or ICU’s for enrollment during the period.
Reopening International Borders
The Caribbean has scored fairly well in “round one”. However, repercussions loom for our fragile, tourism-dependent Caribbean economies. The Caribbean is now embarking on phased, cautious, re-openings of international borders to tourism with strict public health protocols and procedures [8, 9]. Many islands/territories, have been re-opening their international borders during May through July, these include Guyana, Antigua and Barbuda, Jamaica, St Barthelemy, St Lucia, United States’ Virgin Islands, Anguilla, Aruba, Bahamas, Barbados, Bermuda, Dominican Republic, Guadeloupe, Puerto Rico, Sint Martin, St Vincent, the Grenadines, Turks and Caicos. In August, Belize and Grenada plan to open their borders. While Aruba, Bonaire, Curacao, Cuba, Dominica, Haiti, Martinique, Monserrat, St Kitts and Nevis, St Maarten, Suriname, Trinidad and Tobago, remain closed, indefinitely. Visitors are being welcomed and nationals are being repatriated. There are trainings of hundreds of local service providers in hotel, tourist and related industries. Risk assessments, travel cards, screens, thermal scans, quarantine, masking, physical distancing are being evaluated and required at ports of entry. The Bahamas, Barbados, Jamaica, St. Lucia, Antigua, Barbuda and other islands require incoming passengers to submit a negative SARS-CoV-2 PCR test before arrival. Cuba is physically separating its tourists from their residents on outer islands. Jamaica is “Geo-fencing tourists”, on the “Coronavirus Resilient Corridor” of popular tourist spots, using the “Jam-COVID App” for tracking through wrist-bands and cell phones.
Reopening Communities
“Simultaneously, Caribbean communities are gradually re-opening hotels, restaurants, parks, beaches, rivers, bars, churches, businesses, schools, retail stores, hair salons and barber shops. Gatherings have increased from 10, 15, 50 to 125, or more, with physical-distancing. Curfews remain, in some countries. As in health care, several regional and national policies are guiding this process (9). This occurs amidst the raging COVID-19 pandemic nearby in North, Central and South America with genuine concerns for surges and the “second wave” of COVID-19. The Caribbean is still aiming for the best possible outcomes, in “Balancing lives and livelihoods”.
Abbreviations
COVID-19: Novel Coronavirus Disease 2019
GDP: Gross domestic product
CARICOM: Caribbean Community
PAHO: Pan American Health Organization
CARPHA: Caribbean Public Health Agency
CDC: United States’ Centers for Disease Control and Prevention
UWI: University of the West Indies
UHWI: University Hospital of the West Indies
SARS-CoV-2: Severe acute respiratory syndrome coronavirus 2
PCR: Polymerase chain reaction
ICU: Intensive care unit
L/min: Liters per minute
MBBS: Bachelor of Medicine, Bachelor of Surgery
DM: Doctorate in Medicine
MPH: Masters in Public Health
FRCP: Fellow of the Royal College of Physicians
DrPH: Doctorate in Public Health
Declaration
Acknowledgement
Co-authors acknowledge support of the Chief Medical Officers of Health of the Caribbean, the Caribbean Public Health Agency (CARPHA), Pan American Health Organization (PAHO), University of the West Indies (UWI), University Hospital of the West Indies (UHWI). We are grateful to Caribbean’s health care workers, involved in the prevention, treatment and care of patients with COVID-19. We are grateful to the Commonwealth Medical Association and the University of Toronto, to whom this work was first orally-presented, in part, on July 1 and July 31, 2020, respectively.
Ethics approval, availability of data and materials
These data are publicly available, delinked to personal identifiers from WHO / PAHO / CARPHA and /or individual countries, in the context of mandatory reporting, during a global pandemic. Ethics approval was not sought to perform this study.
Funding
This work was funded by the governments of Caribbean countries/ territories who sought support for the COVID-19 response. The authors cannot attest to the source, or quantity of these contributions. The authors did not receive any personal or academic funding to support any of this work.
Author’s contributions
This manuscript was prepared and orally-presented, in part, by Celia DC Christie, at the Commonwealth Medical Association (CMA) Webinar, supported by the Commonwealth Secretariat and World Health Organization (WHO), on “Regional Clinical Management of COVID-19: Perspectives from Canada, W. Africa, the Caribbean, E. Africa, Asia and Europe”, 1 July, 2020. It was updated and represented to the University of Toronto’s academic community, 31 July, 2020. Celia DC Christie conceptualized, drafted, wrote and edited this manuscript. Tamara Thompson contributed to the clinical aspects of the manuscript. Karen Webster-Kerr contributed to the public health aspects of the manuscript. All three co-authors read several drafts and provided their editorial input and approval into the final manuscript, submitted herein for publication.
References
- Ian R Hambleton, Selvi M Jeyaseelan, Madhuvanti M Murphy (2020) COVID-19 in the Caribbean small island developing states: lessons learnt from extreme weather events. Lancet Global Health 8: E1114-E1115. [View]
- Mooney H and Zegarra MA (2020) Extreme Outlier: The Pandemic’s Unprecedented Shock to Tourism in Latin America and the Caribbean. International-American Development Bank. [View]
- Lopez. Ana M (2020) Latin America & Caribbean: travel & tourism contribution to GDP 2010–2019. Statista July 13, 2020. [View]
- Clark A, Jit M, Warren-Gash C, Guthrie B, Wang HH, et al. (2020) Global, regional, and national estimates of the population at increased risk of severe COVID-19 due to underlying health conditions in 2020: a modeling study. Lancet 8: E1003-E1017. [View]
- Pan American Health Organization (2019) NCDs at a Glance: NCD Mortality and Risk Factor Prevalence in the Americas. Washington, D.C. PAHO 2019. [View]
- Pan American Health Organization (2019) Core Indicators 2019: Health Trends in the Americas. Washington, D.C.: PAHO; 2019. [View]
- Knight-Madden J, Lee K, Elana G, Elenga N, Marcheca-Teruel B, et al. (2019) Newborn Screening for Sickle Cell Disease in the Caribbean: An Update of the Present Situation and of the Disease Prevalence. Int Jour Neon Screen 5: 5. [View]
- WHO Coronavirus Disease (COVID-19) Situation Reports. [View]
- Caribbean Public Health Agency (CARPHA) Situation Reports. Coronavirus Disease (COVID-19) Pandemic. [View]
- Countries in the world by population. [View]
- International-American Development Bank. [View]
- WHO – COVID-19 report for July 8, 2020. [View]
- World Health Organization. (2020). Clinical management of severe acute respiratory infection (SARI)when COVID-19 disease is suspected: interim guidance, 13 March 2020. World Health Organization. [View]
- World Health Organization. (2020). Clinical management of COVID-19: interim guidance, 27 May, 2020. World Health Organization. [View]
- Murphy MM, Jeyaseelan SM, Howitt C., Greaves N., Harewood H., Quimby KR, et al. (2020) COVID-19 containment in the Caribbean: The experience of small island developing states. Research in Globalisation 2: 100019. [View]
- Penarrubia L, Ruiz M, Porco R, Rao SN, Juanola-FalgaronaM, Manissero D, et al. (2020) Multiple assays in a real-time RT-PCR SARS-CoV-2 panel can mitigate the risk of loss of sensitivity by new genomic variants during the COVID-19 outbreak. Int J Infect Dis 97: 225–229. [View]
- Tomlin Paul, et al. COVID-19 Pandemic Preparedness Conference. Youtube. 5 March, 2020, by UWI Mona Media. https://www.youtube.com/watch?v=i0Z9Za6ofi8
- Ranucci M, Ballotta A, Di Dedda U, Bayshnikova E.,Dei Poli M., Resta M., et al. The procoagulant pattern of patients with COVID?19 acute respiratory distress syndrome Journal of Thrombosis and Haemostasis, 2020:18; 7: 1747–1751.
https://doi.org/10.1111/jth.14854 - Pan American Health Organization / World Health Organization. Epidemiological Alert: Complications and Sequelae of COVID-19. 12 August 2020, Washington, D.C.: PAHO/WHO; 2020. https://www.paho.org/en/documents/epidemiological-alert-complications-and-sequelae-covid-19-12-august-2020
- Becker R. COVID-19 update: COVID-19-associated coagulopathy. Journal of Thrombosis and Thrombolysis. 2020 May 15:1–14. doi: 10.1007/s11239-020-02134-3
- Mangalmurti N., Hunter CA. Cytokine Storms: Understanding COVID-19. Immunity 2020 Jul 14; 53(1): 19–25. doi: 10.1016/j.immuni.2020.06.017
- https://www.gilead.com/purpose/advancing-global-health/covid-19/voluntary-licensing-agreements-for-remdesivir
- WHO the Solidarity Trial. Coronavirus Update # 22. https://www.who.int/docs/default-source/coronaviruse/risk-comms-updates/update-22-epi-win-covid19.pdf?sfvrsn=a9b4bf6c_4
- Countries in the world by population. [View]
- Pan American Health organisation Situation Report COVID-19 in Jamaica. [View]
- https://theconversation.com/coronavirus-response-why-cuba-is-such-an-interesting-case-135749 April 15, 2020
- https://today.caricom.org/2020/06/23/statement-by-the-organisation-of-eastern-caribbean-states-on-cuban-medical-brigades/ June 23, 2020
- Rouzier V, Liautaud B and Deschamps MM (2020) Facing the monster in Haiti. N Engl J Med 383: 4. [View]
- King A, Andrus JK, Figueroa JP (2020) Financial crisis at PAHO in the time of COVID-19: a call for action. Lancet 6736; 31489–6. [View]